
Fellow Chalk Talk: Dysphagia w/ Dr. Sprague
/Objectives:
Differential orapharyngeal dysphagia from esophageal dysphagia
Develop a differential for esophageal dysphagia
Identify different modalities of evaluation for dysphagia
Video:
Questions from Talk:
+ How exactly does the GERD cause motility issues?
It is not a completely understood pathophysiology, and we're stuck in a which came first the chicken or egg situation. One theory is that the presence of acid in the esophagus irritates the neurons causing dysmotility. Another is that the dysmotility is the cause of the GERD in the first place. Regardless, PPIs help both symptoms when GERD is associated with dysphagia.
+ Why do Schatzki Rings / other strictures recur after dilations?
One reason is undertreatment, i.e. underdilation of the strictures, as there is some associated risk with over dilation - esophageal perforation. Otherwise, if the underlying condition has not been treated, the strictures could recur.
+ Could you speak to the dreaded complication of dysphagia - food impaction? When is it an emergency?
A cardinal symptom to look for when evaluating these patients is if they can tolerate their own saliva. Surprisingly, not all patient's notice that they are constantly spitting. If you see a patient with a spit-bag in the ED, this is sign that they need an EGD sooner rather than later.
+ Any role for chronic PPI in EOE?
If they response to PPIs, they are left on chronic treatment. Otherwise, if they do not respond, you proceed to diet changes and swallowed budesonide.
+ I think we always see people with DES presenting with chest pain but is that typical? Outside of 6S do they present with dysphagia? If so what age/risk factors?
True DES is a rare and you need to do advanced motility and pH studies to diagnose it. Most often, chest pain associated with a GI pathology is going to be undiagnosed GERD rather than DES.
+ Any role for erythromycin for motility issues?
Erythromycin has no utility with esophageal dysphagia. It is most often used for gastroparesis. However, due to the issues with chronic antibiotic use and significant tachyphylaxis, it is not used chronically in patients with gastroparesis. Sometimes it is used for gastric contents clearnace prior to an endoscopy for a UGIB, to help clear the stomach of blood and improve visualization.
+ What do you recommend for patient that have had a gastric sleeve?
Patients with known dysphagia should not have a gastric sleeve. They should have a Roux-en-Y instead. However, post gastric sleeve patients can present with dysphagia not due to esophageal pathology but due to gastric changes of unclear pathophysiology. Treatment involves dilation of the pylorus and the anastomosis near the antrum.
Submit additional questions and we will have our expert answer them
Additional Resources:
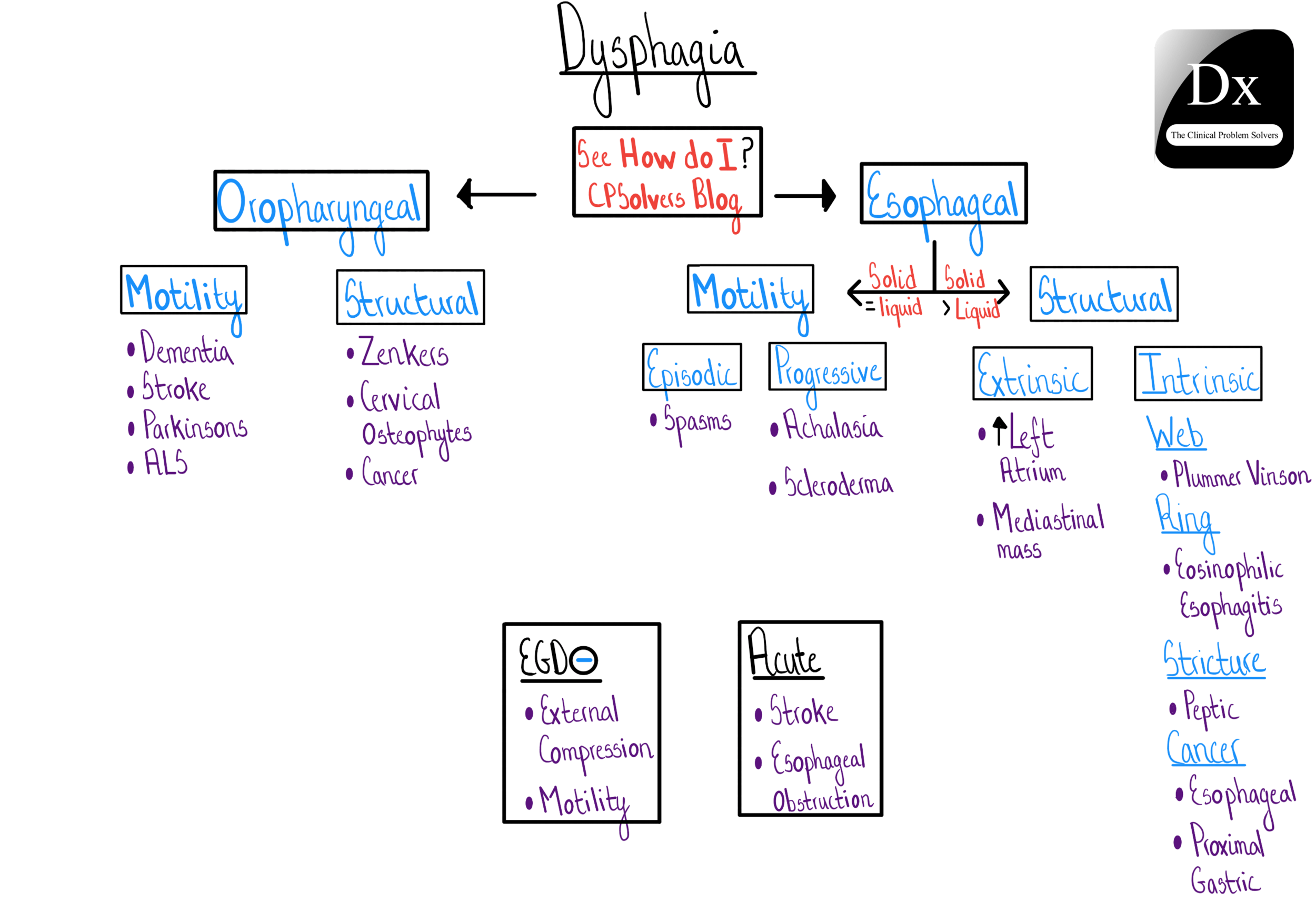
This written as a reference for internists and the first diagram is an excellent schema to think about dysphagia.
Dr. Kahrilas is the world expert on esophageal motility, so he gets into the weeds here. Unless any of you are particularly interested in motility disorders, I would stop reading after the diagram on page 4.
Clinical Problem Solver’s Schema for Dysphagia
MKSAP 18 Questions:
GI Question 5
GI Question 7
GI Question 13
GI Question 56
GI Question 70
Request a Fellow or Faculty for the next Chalk Talk
**As always, contact Gene (novikoyy@ucmail.uc.edu) if you’re interested in helping with out distanced learning.